| 0099-2399/94/2001-0022/$03.00/0 | |
| JOURNAL OF ENDODONTICS Copyright © 1994 by The American Association of Endodontists |
Printed in U.S.A. VOL. 20, No. 1, JANUARY 1994 |
Apical Dentin Permeability and Microleakage Associated with Root End Resection and Retrograde Filling
Peter A. Gilheany, MDSc, David Figdor, MDSc, FRACDS, Dip Endo, and Martin J. Tyas, BDS, PhD, GradDipHlthSc, AFCHSE, FADM
This study evaluated the apical leakage associated with various depths of retrograde fillings placed in root apices which had been resected at one of three different angles. Leakage was assessed with a hydraulic conductance apparatus. Teeth were divided into groups corresponding to the angle of apical resection (0, 30, and 45 degrees to the long axis of the root) and apical leakage was determined following incremental increases in the depth of the retrograde filling (Ketac Silver). Increasing the depth of the retrograde filling significantly decreased apical leakage; there was also a significant increase in leakage as the amount of bevel increased. Both the permeability of resected apical dentin and micro-leakage around the retrograde filling material had a significant influence on apical leakage.
The goal of endodontic therapy is the elimination of bacteria from the root canal system and the subsequent establishment of an effective barrier to prevent further passage of microorganisms or their products to the periapical tissues. Conventional endodontic treatment has been shown to be successful in about 90% of cases (1). If endodontic therapy fails then retreatment is indicated. If this is not possible, or if retreatment fails, periapical surgery may be required.
Periapical surgery consists of one of, or a combination of, simple curettage of infected or inflamed tissue, removal of an infected or damaged root apex or a retrograde filling to prevent communication between the root canal system and the periapical tissues. Most investigations concerning retrograde fillings have focused either on the biocompatibility of the retrograde filling material or evaluating apical microleakage.
There are potentially two avenues by which leakage can occur at the apex of a root sealed with a retrograde filling. The first is by apical microleakage, that is leakage along the interface between the filling material and the canal wall. The second way is by the flow of fluids and substances along open tubules at the resected root end, that is, via permeable apical dentin. The sum of the leakage along these two pathways may be termed “apical leakage.”
It has been reported that the angle of apical resection may influence root end leakage. In a dye leakage study (2) there was significantly more apical dye penetration in groups where the apical cavity preparations did not extend to the coronal level of the bevel. Tidmarsh and Arrowsmith (3) used scanning electron microscopy to examine the resected root ends of teeth. They suggested, on the basis of the number of dentinal tubules apparently communicating between the resected root face and the root canal, that the angle of the bevel should be kept to a minimum and that the retrograde filling should extend coronally into the canal, at least to the level of the coronal end of the bevel. Both of these studies imply that leakage may be possible through apical dentinal tubules.
In most studies of apical microleakage, the details of the root resection and cavity preparation have not been described accurately, so that only a limited comparison between methods can be made. When the angle of apical resection and/or depth of cavity preparation have been cited they have often been empirical. An angle of 45 degrees to the long axis of the root has been most commonly described (4–7). Many authors (8–11) have used a resection technique that produced a flat (horizontal) root end. Some studies have used 1-mm-deep cavity preparations (7); others have used 2-mm-deep (6, 9, 11) or 3-mm-deep (4, 5, 8) cavities. Arens (12) suggested that after the apex has been reduced, a Class I type cavity approximately 3- to 5-mm deep should be prepared. Importantly, in most of these studies, the point from which cavity depth was measured following root resection has not been specified.
Although many studies have investigated microleakage associated with a retrograde filling, very few have examined the influence of the apical bevel and its relationship to apical dentin permeability (2). The aim of this study was to determine the effect of different angles of apical resection and depths of retrograde filling on apical leakage.
MATERIALS AND METHODS
Determination of Microleakage and Dentin Permeability
Apical microleakage and dentin permeability were measured by assessing fluid flow in a hydraulic conductance apparatus similar to that described by Derkson et al. (13). The apparatus consisted of a closed system in which pressurized phosphate-buffered saline (PBS) with a 0.4% fluorescein dye moved through 1.0-mm internal diameter polyethylene tubing and a 25-µm diameter micropipette from a fluid reservoir to the test specimen. The micropipette contained an air bubble, the movement of which indicated fluid flow, and thus microleakage or dentin permeability in the test specimen. By measuring fluid flow over timed intervals, under constant pressure gradients, it is possible to obtain quantitative measurements for a given specimen (14). Repeated or successive experiments can be performed on the same specimen (8, 13).
Root Preparation
Twenty-seven extracted single-rooted human teeth were selected and stored in saline, for a period of up to 3 wk. The crowns were removed with a diamond disc and water coolant, and the roots were divided into three groups of nine. The apices of all of the roots within a group were resected at one of three different angles (Fig. 1) with respect to the long axis of the tooth: either 0 degrees (commencing lingually 2 mm from the anatomical apex), 30 degrees or 45 degrees (both commencing lingually 1 mm from the anatomical apex).
The pulp canal was debrided with K files and 1% sodium hypochlorite. Canal preparation was completed with a #4 Gates Glidden bur throughout the length of the canal. The coronal section of the canal was flared with a #5 Gates Glidden bur to a depth of approximately 2 mm. Smear layer was not deliberately removed in the canal or at the resected apex.
Controls
The resected apical surface of the root was occluded with a sheet of plastic (approximately 15-mm square × 1-mm thick) cemented with cyanoacrylate. The canal was filled with PBS/dye solution and the root cemented with cyanoacrylate to a piece of Plexiglas (1-cm square × 0.7-mm thick), which had an 18-gauge stainless steel tube protruding approximately 2 mm on the root side and 10 mm on the apparatus side. PBS/dye solution was placed into the 18-gauge stainless steel tube, before attachment to the hydraulic conductance apparatus. The entire system was pressurised to 110 kPa and recordings of the position of the bubble were made every minute over a 5-min period. The procedure was repeated for each root, and this leakage measurement was used as the control. All tests were performed at 23 ± 1°C. At the completion of the test period the root segment was detached and stored in PBS. Any roots exhibiting leakage through accessory canals were excluded from the study.
Placement of the Retrograde Filling
After recording a control measurement, the first increment of a glass ionomer filling, Ketac Silver (Espe, Seefeld, Germany), was placed. The canal was dried and a metal stop was positioned approximately 1 mm short of the buccal aspect of the apical resection upon which the Ketac Silver was condensed and allowed to set for at least 5 min before the root was replaced in PBS. Two radiographs, buccolingual and mesiodistal, were taken of each root and the depth of the filling was measured from the buccal aspect of the cavity (Fig. 2, positiion b). The root segment was reattached to the Plexiglas and measuring apparatus, as described for the control, and the leakage was measured.
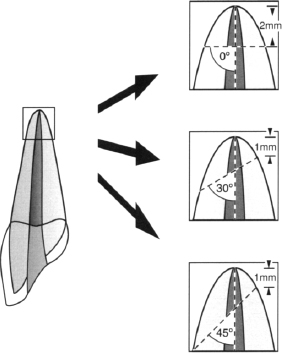
FIG 1. Resection angles of the root apex.
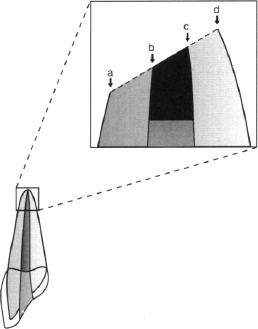
FIG 2. Possible locations from which the retrograde filling depth can be measured: a and b, buccal side of the root and cavity; c and d, palatal side of the cavity and root, respectively.
Further increments of Ketac Silver were added by placing mixed Ketac Silver into a syringe with a blunted 19-gauge needle. The canal was dried, the needle placed into the root to the desired depth, Ketac Silver injected, and compacted against the previous filling. Two radiographs were again taken, and the new filling depth was measured. The root segment was attached to the Plexiglas and the apparatus, and another leakage test was carried out over 5 min. Further increments of Ketac Silver were added until leakage results were similar to those of the control measurement. Between each increment of retrograde filling, the roots were separated from the Plexiglas and stored in PBS.
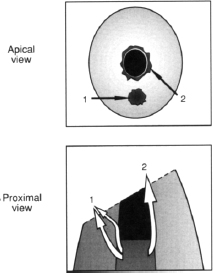
FIG 3. Areas where leakage was observed. Apical view shows leakage on the resected dentin (1) and at the filling-tooth interface (2). Proximal view shows the potential pathways for fluid flow.
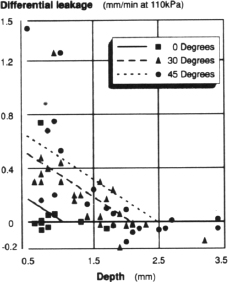
FIG 4. Graph showing differential leakage versus depth of the retrograde filling, including the line equation, for each angel of root resection. Line equation was derived with Y = leakage, D = depth, and B = slope of best fit straight line.
Statistical Analysis
Data collected from each tooth were expressed as differential leakage—the difference between the control (resected end occluded) and experimental (retrograde filling in place) values for leakage. The statistical validity of the results was determined using an analysis of covariance with depth as the covariate. A nested design (hierarchical) with teeth nested within groups and using depth as the covariate was also used. Results were further analyzed by multiple regression using dummy variables to identify groups. A line equation for each group was derived which was compared using linear regression for statistical differences.
RESULTS
In many cases dye leakage could be seen at the apex of the experimental tooth in one of two places, at the tooth-restoration interface or on the beveled surface, to the buccal of the retrograde filling (Fig. 3).
The leakage measurements for controls and following placement of the retrograde fillings are shown graphically in Fig. 4. Analysis of covariance revealed that there were significant differences in leakage between retrograde fillings in teeth resected at 0, 30, and 45 degrees to the long axis of the tooth. Analysis of both response variables showed that increasing the depth of the retrograde filling significantly decreased apical leakage (p ≤ 0.0001) and that there was a significant increase in apical leakage as the amount of the bevel increased (p ≤ 0.001).
The line equation for each group was determined using the formula:
Y = A + BD
where Y = apical leakage, A = constant, B = slope, and D = depth of retrograde filling. (Note. “Slope” refers to Fig. 4, not to the slope of the bevel.) The constant term for each group was determined, and statistical differences were evaluated using linear regression. Statistical differences were found between the 0-degree group and both the 30-degree (p ≤ 0.002) and the 45-degree (p ≤ 0.0001) groups. No statistically significant differences were found between the 45- and 30-degree groups (p ≤ 0.1002).
No significant difference was found between the slopes of each group, so a constant slope term was used. The equation for each group was derived, thus: for the 0-degree group, Y = 0.3315 – 0.3195 D; for the 30-degree group, Y = 0.6661 – 0.3195 D; and for the 45-degree group, Y = 0.798 – 0.3195 D.
DISCUSSION
The purpose of placing a retrograde seal after apicectomy is to establish an effective barrier between the root canal and the periapical tissues when a conventional orthograde seal is not possible or is suspected to be less than intact. Apart from selecting the sealing material, two factors which are under the direct control of the operator are the depth of retrograde filling and the angle of resection. This study showed that increasing the depth of a retrograde filling decreased apical leakage and increasing the bevel increased apical leakage. There was evidence for a contribution from both apical microleakage around the retrograde filling as well as the permeability of resected dentin to overall apical leakage.
As the bevel of the resection changed from 0 degrees to the long axis of the root to 30 degrees and then 45 degrees, the leakage rose significantly. It is reasonable to infer that the increased leakage was primarily due to leakage through permeable apical dentin since a resection angle of 30 or 45 degrees exposes many more dentinal tubules than a flat, 0-degree, cut. If microleakage around the retrograde filling was the sole contributing factor to apical leakage, then the leakage would have been similar in all groups for the same depth of retrograde filling. This, however, was not the case. For example, the differential leakage of a 1-mm deep retrograde filling for the 0-, 30-, and 45-degree groups, as determined from the line equation, was 0.012, 0.347, and 0.478 mm/min at 110 kPa, respectively. Thus, apical leakage cannot be solely a function of the microleakage around the retrograde filling. The concept that there is some leakage through permeable apical tubules is consistent with the direct observation of dye on the beveled surface (Fig. 3) and supports previous suggestions (2, 3) that placing a bevel will increase apical dentin permeability.
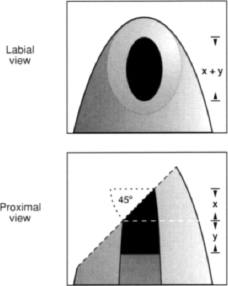
FIG 5. Two views of a retrograde filling. Labial view shows the depth of the filling (x + y) as seen in a clinical radiograph. Proximal view reveals the effective depth as y only.
When the depth of the retrograde filling was progressively increased for each of the specified angles of resection, the apical leakage decreased. We infer that this is due to a reduction in apical microleakage around the retrograde filling as well as to occlusion of many apical tubules that might have been available for passage of fluid to the apex.
The open tubules of the resected root end may provide a potential route of communication for the contents of the root canal into the periapical tissues and this implies that an important function of the retrograde filling must be to seal the permeable dentinal tubules as well as the root canal. This has been shown experimentally, utilizing cavity varnish applied on the resected apex, to be highly effective in reducing apical leakage (4). A clinical technique based on this principle, in which the entire resected apex is covered with a dentinbonded composite, has recently been described (15).
The optimum depth of the retrograde cavity required to minimize apical leakage can be determined by utilizing the equations derived from the regression analysis of the data. Here, the optimum leakage is considered to be zero. Thus, for teeth resected at 0 degrees to the long axis, the depth of the retrograde filling is 1.0 mm for zero leakage. Similarly, teeth with apicectomies of 30 and 45 degrees require a retrograde filling depth of 2.1 and 2.5 mm, respectively, for zero leakage. Our data also point to the fact that increasing the depth of the retrograde filling beyond that described above will not further reduce apical leakage. This confirms previous studies involving a flat (0-degree) resection where there was no significant difference in leakage between a 1-mm and 4-mm-deep amalgam (16) or between a 1-mm and 3-mm-deep amalgam at 27 days after insertion (10), although there was a significant difference prior to 25 days (10).
There are several factors to consider in relating these findings to the clinical case. First, the ideal angle of resection is a flat (0-degree) cut since this minimizes apical leakage. However, the requirement for good surgical access when placing a retrograde filling means that a resection with at least some bevel is often necessary and in this case it should be kept to the smallest angle possible. The angle at which the tooth may be proclined in the alveolus should also be taken into account when the apex is actually resected. Second, radiographic angulation may result in distortion of the radiographic image of the retrograde filling, thus affecting the perceived length of filling. Third, evaluating the depth of the retrograde filling from a radiograph may lead the operator to misinterpret the real depth of the filling. For example, Fig. 5 shows that the effective depth of the retrograde filing would be y. However, in a clinical radiograph, the depth would appear as x + y. If the bevel was 45 degrees, and the diameter of the retrograde filling was 1 mm, the effective depth would be 1 mm less than the depth as measured on a radiograph. For this reason, and since it is also clinically difficult to evaluate the angle of the bevel, the retrograde filling on a beveled resected apex should ideally be 3.5-mm deep (when measured radiographically) for minimal apical leakage.
Most model systems used for measuring microleakage and dentin permeability do not completely reproduce the in vivo environment (17). It is not known whether or not the factors evaluated here may alter the success rate of clinical treatment; however, since the treatment goal is to minimize the possibility of bacteria and their metabolites exiting the root canal system and gaining entry to the periapical tissues, any factor which may improve the seal between the canal and the periapical tissues should be utilized.
This study has shown that increasing the depth of the retrograde filling significantly decreased apical leakage and that there was significant increase in leakage as the amount of bevel increased, due to leakage through the resected apical dentin. The optimum depths for a retrograde cavity (measured from the buccal aspect of the cavity) are 1.0, 2.1, and 2.5 mm for 0-, 30-, and 45-degree angles of resection, respectively. Apical leakage can be minimized by resecting the root apex at an angle of 0-degrees to the long axis. Finally, when measured in vitro, the permeability of the resected apical dentin and microleakage around the retrograde filling material both have a significant influence on apical leakage.
This research was supported by a grant from the Australian Society of Endodontology, Inc.
The authors thank Dr. David Pashley for providing the hydraulic conductance apparatus and Professors Sundqvist and Messer for valuable criticism of the manuscript.
Drs. Gilheany, Figdor, and Tyas are affiliated with the School of Dental Science, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, 711 Elizabeth Street, Melbourne, Australia. Address requests for reprints to Dr. Peter Gilheany, 424–426 Nepean Highway, Frankston, 3199 Australia.
References
1. Sjögren U, Hägglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endodon 1990;16:498–504.
2. Beatty R. The effect of reverse filling preparation design on apical leakage [Abstract 805]. J Dent Res 1986;65:259.
3. Tidmarsh BG, Arrowsmith MG. Dentinal tubules at the root ends of apicected teeth: a scanning electron microscopic study. Int Endod J 1989;22:184–9.
4. Vertucci FJ, Beatty RG. Apical leakage associated with retrofilling techniques: a dye study. J Endodon 1986;12:331–6.
5. Schwartz SA, Alexander JB. A comparison of leakage between silver glass ionomer cement and amalgam retrofillings. J Endodon 1988;14:385–91.
6. Zetterqvist L, Anneroth G, Danin J, Röding K. Microleakage of retrograde fillings—a comparative investigation between amalgam and glass ionomer cement in vitro. Int Endod J 1988;21:1–8.
7. Yoshimura M, Marshall FJ, Tinkle JS. In vitro quantification of the apical sealing ability of retrograde amalgam fillings. J Endodon 1990;16:9–12.
8. King KT, Anderson RW, Pashley DH, Pantera EA. Longitudinal evaluation of the seal of endodontic retrofillings. J Endodon 1990;16:307–10.
9. Szeremeta-Browar TL, Van Cura JE, Zaki AE. A comparison of the sealing properties of different retrograde techniques: an autoradiographic study. Oral Surg 1985;59:82–7.
10. Mattison GD, von Fraunhofer JA, Delivanis PD, Anderson AN. Micro-leakage of retrograde amalgams. J Endodon 1985;11:340–5.
11. Thirawat J, Edmunds DH. The sealing ability of materials used as retrograde root fillings in endodontic surgery. Int Endod J 1989;22:295–8.
12. Arens DE. Surgical endodontics. In: Cohen S, Burns RC, eds. Pathways of the pulp. 4th ed. St. Louis: CV Mosby, 1987.
13. Derkson GD, Pashley DH, Derkson ME. Microleakage measurement of selected restorative materials: a new in vitro method. J Prosthet Dent 1986; 56:435–40.
14. Pashley DH. Dentin permeability: theory and practice. In: Spångberg L, ed. Experimental endodontics. Boca Raton, FL: CRC Press Inc., 1990.
15. Rud J, Munksgaard EC, Andreasen JO, Rud V. Retrograde root filling with composite and a dentin-bonding agent. 2. Endod Dent Traumatol 1991; 7:126–31.
16. Edmunds DH, Thirawat J. The sealing ability of amalgam used as a retrograde root filling in endodontic surgery. Int Endod J 1989;22:290–4.
17. Trowbridge HO. Model systems for determining biologic effects of microleakage. Oper Dent 1987;12:164–72.
You Might Be Interested
After correcting for all other factors, a recent study showed that those who have engaged in vigorous physical activity for a prolonged period some time in their lives have a considerably reduced risk of stroke (Br Med J 307:232 1993).
For persons older than 55 years of age who had exercised only between ages 15 and 25, the rate of stroke was one half that of someone who never exercised. Those who continued vigorous exercise from ages 15 to 55 had one quarter the stroke risk of perpetual couch potatoes.
“Use it or lose it” can now be expanded to “use your body or lose your brain.”
David Bishop